The QUATTRO is one of the most flexible, efficient and compact lasers on the market. Many metal working companies have a large number of components to manufacture but only need to produce one or two at a time. Ease of use, plus low operating costs make the QUATTRO the ideal solution for low volumes, without forgoing precision and quality.
This machine is no longer available.
Find the laser machine that suits your needs
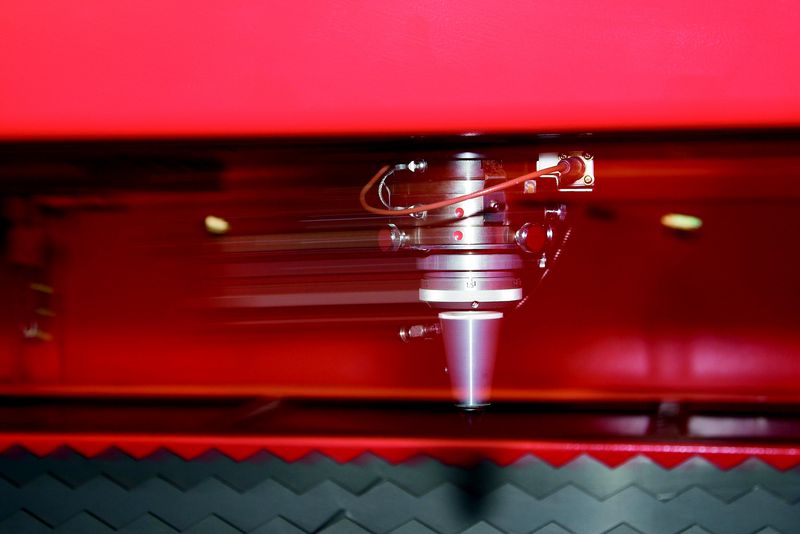
FULL ACCESS TO THE CUTTING AREA:
The three accessible sides of the QUATTRO laser facilitate sheet metal loading and unloading. Large-sized sheets which are bigger than the work area can also be processed, repositioning them manually.

COMPACT STRUCTURE:
With a footprint of just 6.4 m2, the QUATTRO is AMADA's smallest laser. The oscillator and numerical control are contained within the machine to maintain its extremely compact size.

DIVERSIFIED PROCESSING:
With the QUATTRO, not only sheet metal but rectangular and square tubes can be processed, providing even greater flexibility. (Option)

FULL ACCESS TO THE CUTTING AREA:
The three accessible sides of the QUATTRO laser facilitate sheet metal loading and unloading. Large-sized sheets which are bigger than the work area can also be processed, repositioning them manually.
COMPACT STRUCTURE:
With a footprint of just 6.4 m2, the QUATTRO is AMADA's smallest laser. The oscillator and numerical control are contained within the machine to maintain its extremely compact size.
DIVERSIFIED PROCESSING:
With the QUATTRO, not only sheet metal but rectangular and square tubes can be processed, providing even greater flexibility. (Option)
| QUATTRO | QUATTRO | |
|---|---|---|
| Laser power (W) | 1000 | 2500 |
| Machine type | CO₂ flying optic laser | CO₂ flying optic laser |
| Working range X x Y (mm) | 1250 x 1250 | 1250 x 1250 |
| Working range Z-axis (mm) | 100 | 100 |
| Table loading weight (kg) | 80 | 160 |
Material thickness (max.)*: | ||
| - Mild steel (mm) | 6 | 12 |
| - Stainless steel (mm) | 2 | 5 |
| - Aluminium (mm) | 1 | 4 |
Dimensions: | ||
| Length (mm) | 2900 | 2950 |
| Width (mm) | 2450 | 2450 |
| Height (mm) | 2160 | 2160 |
| Weight (kg) | 3750 | 4150 |
* Maximum thickness value depends on material quality and environmental conditions
Technical data can vary depending on configuration / options
Please contact us for more details and options or download our brochure

For your safe use.
Be sure to read the user manual carefully before use.
When using this product, appropriate personal protection equipment must be used.

Laser class 1 when operated in accordance to EN 60825-1
Increasingly, academic medical centers and evidence-based practices are adopting selected functional markers (e.g., vitamin D, hs-CRP, omega-3 index, insulin resistance indices like HOMA-IR). The challenge remains standardization of optimal ranges and inter-lab variability for specialized tests (e.g., stool PCR versus culture). Laboratory evaluations in integrative and functional medicine represent an expansion—not a rejection—of conventional clinical pathology. By shifting from population-based reference ranges to individualized optimal ranges, from static snapshots to dynamic rhythms, and from disease-focused cutoffs to functional matrix mapping, these tests illuminate the hidden terrain of subclinical dysfunction. When paired with a detailed clinical history and used judiciously, functional labs empower both patient and practitioner to address root causes rather than suppressing symptoms. The PDFs and manuals that detail these evaluations are valuable references, but their true power lies in the interpretive art—seeing patterns, not just numbers, in the service of restoring whole-person health. For a specific PDF document, please check sources such as the Institute for Functional Medicine’s (IFM) “Functional Medicine Laboratory Toolkit,” Genova Diagnostics, or the DUTCH test website, where many overview documents are freely available as PDF downloads. You may also search your academic library or PubMed Central for review articles on “biomarkers in functional medicine.”
Integrative and functional medicine (IFM) represents a paradigm shift from conventional disease-centered diagnosis to a patient-centered, systems-biology approach. In this model, laboratory evaluations are not merely tools for identifying pathology but are instead used to uncover underlying physiological imbalances, optimize function, and prevent chronic disease. Unlike conventional testing, which often asks, “Is this lab value abnormal?” functional medicine asks, “Is this value optimal for this individual’s health and resilience?” This essay explores the philosophy, key testing modalities, and interpretive frameworks that define laboratory evaluations in integrative and functional medicine. Foundational Philosophy: From Diagnosis to Function Conventional laboratory reference ranges are typically derived from population statistics (often the central 95% of a presumably “healthy” population), meaning 1 in 20 healthy individuals will fall outside the normal range, and many subclinical dysfunctions remain within the statistical norm. Functional medicine uses optimal ranges —narrower, physiologically-based targets associated with low disease risk and high performance. For example, a conventional lab may report a fasting glucose of 95 mg/dL as “normal,” while functional medicine would flag this as early insulin resistance, targeting an optimal range of 70–85 mg/dL. For a specific PDF document, please check sources
Furthermore, functional labs prioritize over static levels. Instead of a single thyroid-stimulating hormone (TSH) measurement, functional assessment may include a full thyroid panel (free T3, free T4, reverse T3, and thyroid antibodies) along with basal body temperature and symptoms. Instead of a one-time cortisol level, a diurnal cortisol rhythm is mapped via salivary or dried urine testing. Core Categories of Functional Laboratory Evaluations The following laboratory domains are routinely employed in integrative medicine to map the “matrix” of health—a term referring to the interconnected physiological networks. Instead of a one-time cortisol level